
Neuroectodermal tumour treatment is not specified by a single method. There are various causes and different treatment options for these tumours. Neuroectodermal tumours (NETs) are rare, aggressive cancers that arise from neuroectodermal cells—primitive cells of the nervous system. These tumours can occur in the central nervous system, peripheral nerves, or soft tissues. Common examples include medulloblastomas, primitive neuroectodermal tumours (PNETs), and Ewing’s sarcoma. Effective treatment requires a multidisciplinary approach that considers tumour location, stage, age of the patient, and overall health.
What Are Neuroectodermal Tumours?
Neuroectodermal tumours (NETs) are a group of rare, aggressive cancers that originate from neuroectodermal cells, early cells in the developing nervous system. These tumours can occur in the brain, spinal cord, peripheral nerves, or soft tissues. They are most common in children and young adults and include types such as medulloblastomas, primitive neuroectodermal tumours (PNETs), and Ewing’s sarcoma. Because they can grow quickly and spread, timely diagnosis and a multidisciplinary treatment approach are essential for improving outcomes.
Book Appointment
GET A FREE QUOTE
Neuroectodermal Tumours Examples
Neuroectodermal tumours are a diverse group with varying clinical behaviours, locations, and histology. They may occur at any age, but infants are more prone to these conditions. Here are the specific conditions that show Neuroectodermal Tumours.
Each of these tumours demands a specific treatment approach, often combining surgery, chemotherapy, and radiation. Early diagnosis and tailored therapy have a significant impact on survival outcomes. These examples illustrate the complexity and urgency of managing neuroectodermal tumours in both children and adults.
Who is Prone to Neuroectodermal Cancers?
Neuroectodermal tumours primarily affect children, adolescents, and young adults, though they can occur at any age. The risk is higher in individuals with certain genetic syndromes, such as Li-Fraumeni syndrome or neurofibromatosis. Children under the age of 10 are particularly vulnerable to central nervous system tumours like medulloblastoma. Ewing’s sarcoma, a peripheral neuroectodermal tumour, often affects teenagers and young adults, with a slightly higher occurrence in males. Although the exact cause remains unclear, environmental exposures and genetic predisposition may contribute to risk.
- Children and Adolescents: Most commonly affected, especially under 10 years of age
- Young Adults: Especially those with peripheral PNETs like Ewing's sarcoma
- Genetic Syndromes: Conditions like Li-Fraumeni syndrome and neurofibromatosis increase risk
- Gender** Factor:** Slightly higher occurrence in males
- Environmental Exposure: Though not clearly defined, some chemicals and radiation may play a role.
Book Appointment
GET A FREE QUOTE
Different Treatment For Neuroectodermal Tumours- What is the treatment for PNET?
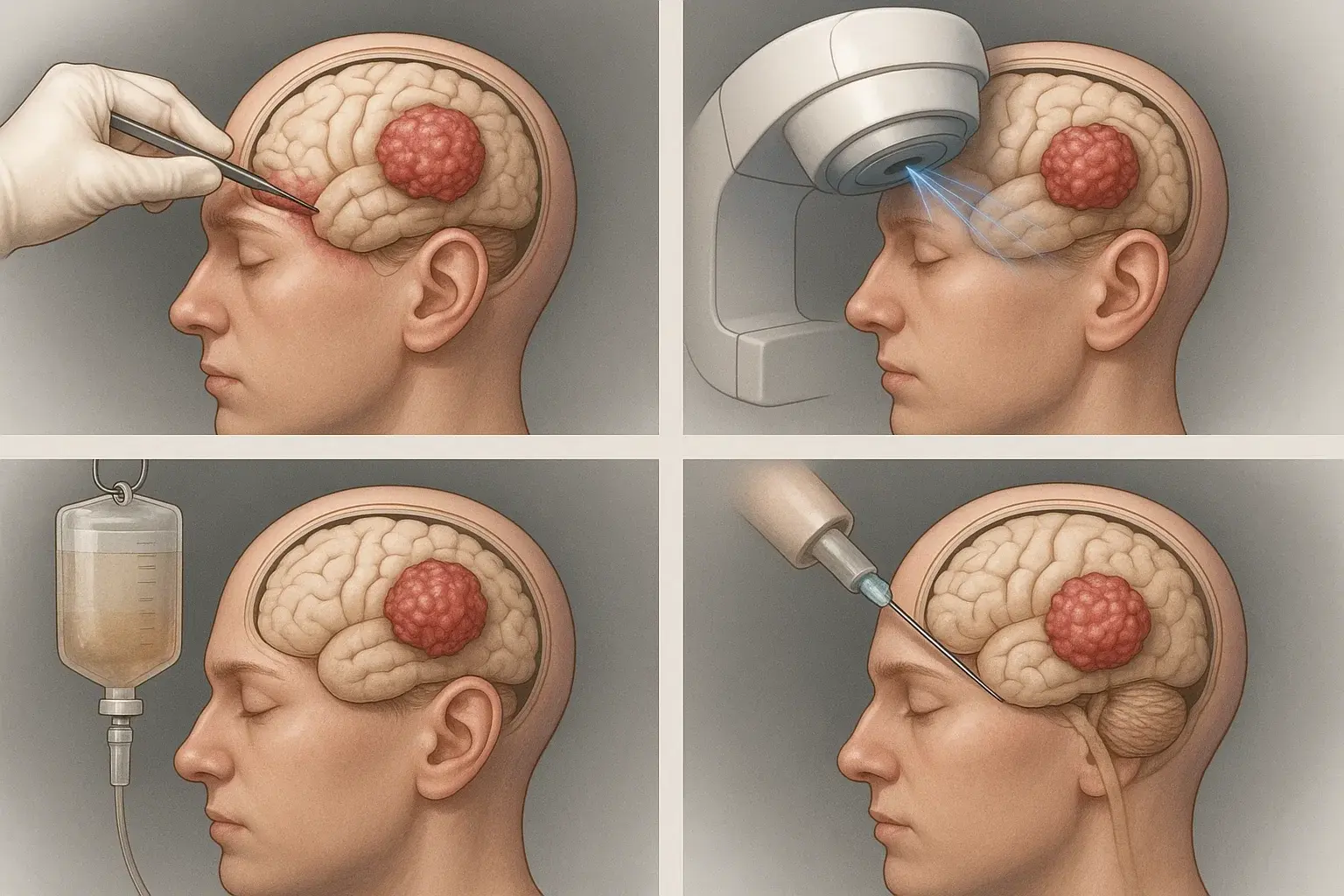
Like other diseases, there are different treatments, such as surgery, chemotherapy, and stem cell implantation. Treatment is often multimodal, combining surgery, chemo, and radiation for the best results. Early diagnosis and personalised treatment plans improve outcomes.
Neuroectodermal Tumours Treatment is combined with several clinical trials and palliative care. Clinical trials are research studies that test new treatments or drug combinations. Here are the different treatment options for Neuroectodermal Tumours (NETs), depending on the type, location, and stage of the tumour:
Hospital For Neuroectodermal Tumours Treatment
There are different hospitals for tumour treatment. They give malignancy-oriented treatment to the patients. Palliative care is provided alongside curative treatment or as the main approach when active cancer treatment is no longer effective. It includes medical, psychological, and supportive services tailored to the patient’s needs and can greatly improve comfort and well-being. For patients with rare, recurrent, or treatment-resistant neuroectodermal tumours, clinical trials provide access to advanced therapies that are not yet available to the general public.
|
Location |
Cities |
|
Tata Memorial Hospital |
Mumbai, Maharashtra |
|
All India Institute of Medical Sciences (AIIMS) |
New Delhi |
|
Apollo Hospitals |
Chennai, Tamil Nadu |
|
Christian Medical College (CMC) |
Vellore, Tamil Nadu |
|
Fortis Memorial Research Institute |
Gurugram, Haryana |
|
Medanta – The Medicity |
Gurugram, Haryana |
|
Rajiv Gandhi Cancer Institute |
Delhi |
|
Kokilaben Dhirubhai Ambani Hospital |
Mumbai, Maharashtra |
|
PGIMER (Postgraduate Institute) |
Chandigarh |
|
Max Super Speciality Hospital |
Delhi |
|
HCG Cancer Centre |
Bangalore, Karnataka |
|
Narayana Health City |
Bangalore, Karnataka |
|
Amrita Institute of Medical Sciences |
Kochi, Kerala |
|
Sir Ganga Ram Hospital |
New Delhi |
|
KIMS (Krishna Institute of Medical Sciences) |
Hyderabad, Telangana |
Cost of Neuroectodermal Tumours Treatment
The total cost of neuroectodermal tumours treatment in India can range from ₹4 lakh to ₹30 lakh or more, depending on tumour complexity, treatment plan, and hospital infrastructure. Public hospitals like AIIMS offer subsidised or free care for eligible patients, while private hospitals may provide premium but costlier services. Advanced treatments like stem cell transplants or targeted therapy significantly increase the overall cost. It’s essential to get a detailed treatment estimate from the chosen hospital and inquire about insurance coverage or financial aid programs.
Book Appointment
GET A FREE QUOTE
|
Estimated Cost (INR) |
Cost in INR |
|
Surgical Tumour Removal |
₹2,50,000 – ₹6,00,000 |
|
Chemotherapy (full cycle) |
₹1,50,000 – ₹5,00,000 |
|
Radiation Therapy (IMRT/IGRT) |
₹1,20,000 – ₹3,50,000 |
|
Stem Cell / Bone Marrow Transplant |
₹10,00,000 – ₹25,00,000 |
|
Targeted Therapy (if applicable) |
₹80,000 – ₹2,50,000/month |
|
Immunotherapy (experimental/optional) |
₹1,50,000 – ₹4,00,000/month |
|
Hospital Stay (per day) |
₹5,000 – ₹15,000 |
|
Diagnostic Tests & Imaging |
₹40,000 – ₹1,00,000 |
|
Follow-up & Supportive Care |
₹20,000 – ₹80,000/year |
We Care Health Services For Neuroectodermal Tumours Treatment
We Care Health Services stands out as a trusted healthcare facilitator offering access to top oncologists, neurosurgeons, and cancer hospitals across India. Their personalised, patient-first approach ensures that individuals battling neuroectodermal tumours receive the best care, right from diagnosis to recovery. They simplify the complex treatment process by coordinating appointments, hospital admissions, second opinions, and follow-ups, making high-quality cancer care accessible, affordable, and less stressful for patients and families.
- Access to Top Cancer Hospitals
Connects patients with India’s leading cancer centres like Tata Memorial, AIIMS, Apollo, and more. - Expert Oncologist Network
Offers referrals to highly experienced specialists in neuro-oncology, pediatric oncology, and advanced surgical oncology. - Affordable Treatment Packages
Helps arrange cost-effective packages for surgery, chemotherapy, radiation, and advanced therapies like stem cell transplant. - Support at Every Step
Full guidance with treatment planning, travel, visa, accommodation, and recovery support—ideal for both Indian and international patients. - Fast Appointments & Second Opinions
Quick coordination for consultations, reducing waiting times and ensuring timely diagnosis and treatment. - Multilingual & Compassionate Team
Provides language support and emotional counselling to ensure patients and families feel understood and cared for. - Tailored Treatment Guidance
Recommends hospitals and specialists based on tumour type, stage, age group (especially pediatric cases), and budget. - Post-Treatment Follow-Up
Assists with long-term care planning, rehabilitation, and lifestyle support after cancer treatment.